Mesothelioma Help Cancer News
American Society of Clinical Oncology (ASCO) releases update to its pleural mesothelioma treatment guidelines
Earlier this year, the American Society of Clinical Oncology (ASCO) published an update to its 2018 guideline for the treatment of pleural mesothelioma. This summary of the guidelines is based on the published manuscript by Kindler HL, Dagogo-Jack I, de Perrot M, Drazer MW, Ismaila N, Hassan R. Treatment of Pleural Mesothelioma: ASCO Guideline Clinical Insights. JCO Oncol Pract. 2025 Mar 7:OP2500035. doi: 10.1200/OP-25-00035. Epub ahead of print. PMID: 40053896.
To update this document, mesothelioma experts from fields of medical oncology, surgery, pathology, radiation oncology and others, convened to review and analyze 110 relevant studies for each recommendation presented. The recommendations were divided into categories such as diagnosis, surgery, immunotherapy, chemotherapy, radiation therapy, pathology, and germline testing.
Researchers and providers who contributed to these treatment guidelines are affiliated with the following centers:
- University of Chicago Medicine
- American Society of Clinical Oncology
- University of California San Diego Moores Cancer Center
- Cross Cancer Institute, University of Alberta
- University of Wisconsin-Madison and Carbone Cancer Center
- Massachusetts General Hospital Cancer Center
- Johns Hopkins University
- Memorial Sloan Kettering Cancer Center
- Princess Margaret Cancer Centre – Toronto, Canada
- Center for Cancer Research, National Cancer Institute
- Levine Cancer Institute
- National Cancer Institute, Egypt
- Mesothelioma Applied Research Foundation
DIAGNOSIS AND STAGING
Mesothelioma patients often present with certain generalized symptoms that don’t go away after treatment. Pleural effusions, an uncomfortable accumulation of fluid in the pleural space that makes it difficult to expand the lung and breathe, are one of the most common symptoms.
Initial Assessment: In patients presenting with fluid, thoracentesis for pleural effusions, followed by cytologic examination is strongly recommended.
Biopsy: Thoracoscopic biopsy is strongly recommended when treatment is planned; use minimal incisions in potential surgical fields.
Alternative Biopsy Methods: Use core needle or open pleural biopsy only when thoracoscopic biopsy is not feasible.
Imaging:
- CT chest/abdomen with contrast and FDG PET/ CT for staging. (FDG is radioactive glucose injected into the bloodstream to see which areas of the tumor are metabolically active and how active they are.
- MRI (optional) to evaluate chest wall / diaphragm / mediastinum invasion.
Invasive Staging: Mediastinoscopy and/or EBUS for PET-avid nodes in candidates for maximal surgical cytoreduction; laparoscopy for suspected abdominal spread.
Measurement & Staging:
- Expert radiologist should perform measurements on CT scan based on modified RECIST 1.1 criteria.
- Follow mRECIST 1.1 for response evaluation; CT-based tumor volume measurement remains investigational.
SURGERY
Mesothelioma surgery has been at the center of debate since the release of the United Kingdom’s phase III study results from the Mesothelioma and Radical Surgery (MARS) 2 randomized controlled clinical trial. This was the first such trial in mesothelioma. The study results showed that patients treated with chemotherapy alone fared better than those who underwent surgery. However, researchers caution that interpretation of the study ought to consider data from nonrandomized surgical studies which show better outcome and much lower 30 and 90-day mortality. As a result, surgery should still be considered for patients with favorable prognostic characteristics.
General Guidance: Surgery should not be based on resectability alone. It’s reserved for select patients with early-stage (T1-3N0), epithelioid histology.
Surgical Options:
- Lung-sparing procedures (PD/EPD) preferred over EPP.
- EPP reserved for exceptional cases at high-volume centers.
Multimodality Care: Surgery should be part of a multidisciplinary approach including chemo/immunotherapy.
Neoadjuvant or Adjuvant Therapies:
- Chemotherapy (pemetrexed/platinum) may be given pre- or postoperatively.
- Neoadjuvant immunotherapy is an option; adjuvant immunotherapy is not recommended due to limited data currently available.
Palliative Surgery: For patients unfit for full cytoreduction, procedures like tunneled catheters or pleurodesis are options.
Intracavitary Therapies: May be safe at experienced centers, but benefits are unclear.
IMMUNOTHERAPY
First-Line Therapy:
- Ipilimumab + Nivolumab is standard for all histologies, particularly nonepithelioid types (CheckMate 743).
- Chemo-immunotherapy (e.g., pembrolizumab + pemetrexed + platinum) is an alternative.
Biomarkers: PD-L1, TMB, and MSI should not guide immunotherapy decisions.
Duration: Up to 2 years unless toxicity or progression.
Second-Line Use:
- Single-agent (e.g., nivolumab) or dual-agent immunotherapy can be used after chemotherapy.
- Retreatment is an option in selected cases.
CHEMOTHERAPY
Chemotherapy was for many years the only standard treatment approved for mesothelioma. This treatment regimen is most familiar to researchers and physicians alike ensuring the most consistent side effect control. However, chemotherapy for mesothelioma has many limitations. For instance, patients with the nonepithelioid subtype do not respond to chemotherapy very well.
First-Line:
- Epithelioid: Pemetrexed + platinum ± bevacizumab.
- Nonepithelioid: Prefer immunotherapy; use chemotherapy only if immunotherapy is contraindicated.
Maintenance: Pemetrexed maintenance not recommended; gemcitabine maintenance may be offered.
Second-Line:
- After immunotherapy: Use pemetrexed + platinum ± bevacizumab.
- After both: Options include gemcitabine ± ramucirumab or vinorelbine.
Special Populations:
- PS 2: Single-agent chemo may be offered.
- PS ≥3: Palliative care recommended.
Duration: 4–6 cycles recommended; break afterward if stable or responding.
RADIATION THERAPY
Radiation therapy for mesothelioma is typically used in conjunction with other treatments to reduce chances of local recurrence. Sometimes, it is also used to shrink tumors as symptom-management.
Prophylactic Radiation: Not recommended to prevent tract recurrence.
Adjuvant Use:
- May reduce local recurrence; recommend in experienced centers.
- Use hemithoracic IMRT post-EPP or post-PD/EPD (preferably in trials).
Palliative Use: Strongly recommended for symptom control using standard regimens.
Neoadjuvant Radiation: Due to potential for severe pulmonary toxicity, neoadjuvant radiation is not recommended with lung-sparing surgery.
Techniques: Use 2D, 3D, IMRT, or electrons depending on tumor site and organs at risk.
PATHOLOGY
The field of pathology is crucial in diagnosing the exact type of tumor in order to help determine the appropriate treatment.
Terminology: Non-malignant mesotheliomas have now been recategorized and renamed, so use of term “mesothelioma” without “malignant” preceding it, is now appropriate.
Diagnostic Tools: IHC with both positive and negative mesothelioma markers.
Subtype Reporting: Required: epithelioid, sarcomatoid, or biphasic, with detailed grading.
Biomarkers: Non-tissue-based biomarkers (e.g., serum tests) are not reliable for monitoring.
MIS (Mesothelioma In Situ): Consider in recurrent unilateral effusions; test with BAP1 and MTAP IHC.

Parp-Inhibitors show promise in mesothelioma treatment
At this year’s American Association for Cancer Research, investigators from the United Kingdom announced the positive results of a mesothelioma clinical trial testing a relatively new class of targeted drugs: the PARP inhibitors.
The study Niraparib Efficacy in Patients With Unresectable Mesothelioma (NERO) enrolled 88 patients randomized into two groups showed that those treated with niraparib extended the median progression-free survival by 1.5 months compared to the arm of patients who only received symptom management care.
Eligible patients had already undergone standard chemotherapy treatment for mesothelioma with success, but they relapsed with the cancer coming back or growing.
Currently, there are no proven therapies for mesothelioma beyond initial treatment and after recurrence. Data on the efficacy of chemotherapy are limited, and immunotherapy retreatment has been only a recent addition to the doctors’ treatment arsenal.
What are PARP inhibitors?
Simply put, PARP inhibitors are drugs that prevent the enzyme known as poly ADP ribose polymerase (PARP) from doing its job of repairing damaged DNA in cells. If not repaired, damaged cells, including cancer cells, die. Conversely, if repaired, even if the repair is erroneous, the cells go on to survive and replicate which can be problematic with cancerous cells. Typically, patients who responded to chemotherapy previously are more likely to see a benefit from this class of drugs. While this study did not require patients enrolled to have a somatic BAP1 deletion, other studies looking into this agent often do. Somatic mutations are those not passed down to offspring and are instead acquired in the cells over time. BAP1 is a tumor suppressor gene, therefore its deletion is understood as consequential in mesothelioma.
Clinical trials employing PARP inhibitors currently available in the United States
While this study took place in the United Kingdom, in the U.S. clinical studies utilizing PARP inhibitors have been available to mesothelioma patients who fit certain eligibility criteria. Currently, one of those studies is still open and enrolling.
Olaparib in Patients with HRD Malignant Mesothelioma is available at the University of Chicago Medicine to patients with the loss of BAP1 and/or a germline (passed down from parents) or somatic (acquired over lifetime) mutation that disrupts protein function in at least one of the patient’s genes.
Could there be another mesothelioma cell type beyond epithelioid, sarcomatoid, and biphasic?
In recent years, mesothelioma histology has become more important than ever, as researchers find that certain treatments are more effective against different cell types. The epitheliod subtype of mesothelioma is by far the most common and is considered the least aggressive of the three types. The sarcomatoid subtype is less common but most aggressive. When a tumor contains both types of cells, it is known as biphasic.
As far as treatment goes, epitheliod mesothelioma tends to respond to chemotherapy better than the sarcomatoid subtype, while benefits of immunotherapy are more pronounced in patients with the more aggressive sarcomatoid subtype.
But now, researchers believe to have identified mesothelioma cells that are neither sarcomatoid nor epitheliod. In the preprint article “Comprehensive multi-site profiling of the malignant pleural mesothelioma micro-environment identifies candidate molecular determinants of histopathologic type,” by Raphael Bueno, MD, et al., the authors suggest that a third category of cells exist in the tumor microenvironment of mesothelioma and are most prevalent in tumors of patients with biphasic disease. Those cells have been named “uncommitted” because the idea is that at some point they might take on an epitheliod or sarcomatoid appearance.
As the researchers examined tumor samples, they noticed that in predominantly epitheliod, and in predominantly sarcomatoid mesotheliomas, such uncommitted cells were few, but in biphasic mesothelioma they were substantial.
Significance of histology (tumor cell type) for mesothelioma patients
The cellular type of the mesothelioma tumor helps doctors determine the prognosis and best treatment for a patient. For example, it is currently known that survival varies depending on the cell type. Patients with epitheliod mesothelioma have the best prognosis, and those with sarcomatoid the worst. The biphasic patients tend to fall in between depending on the proportion of epitheliod vs sarcomatoid cells in their tumors. Moreover, tumor histology helps doctors identify the best treatment for a patient. Sarcomatoid and biphasic tumors have shown the greatest benefit when treated with immunotherapy, and the least benefit when treated with chemotherapy. As mesothelioma research continues to advance, the tumor microenvironment is seen as far more important than individual cells in the proliferation of this cancer.
Because mesothelioma prognosis currently relies so heavily on histology, this discovery adds another layer of nuance to an already complex disease. In addition to understanding the significance and purpose of these uncommitted cells, another question for researchers to untangle in the future will be to understand whether these uncommitted cells ultimately become committed, and whether they commit to the epitheliod or sarcomatoid type and why.
Predicting effectiveness of mesothelioma immunotherapy
In recent years, immunotherapy has revolutionized cancer treatment for most cancers, and even the notably difficult-to-treat mesothelioma has reaped benefits. However, despite two new FDA treatment approvals featuring immunotherapy, this treatment only works for a minority of mesothelioma patients and the benefit is most obvious in the most aggressive, sarcomatoid group. This fact, paired with concerns of immune toxicity, can make some patients and physicians wish they had more tools to gauge if immunotherapy will be more useful than harmful. But are we able to predict its effectiveness before starting treatment?
Drs. Farhad Kosari and Maria Disselhorst of the Mayo Clinic, among others, have been studying exactly this problem. In their paper “Tumor Junction Burden and Antigen Presentation as Predictors of Survival in Mesothelioma Treated with Immune Checkpoint Inhibitors” published in the Journal of Thoracic Oncology, the authors conclude that an analysis of tumor genetics for mutations may facilitate patient selection for immunotherapy treatments based on checkpoint inhibitors.
Why is mesothelioma so difficult to treat?
There are many reasons for mesothelioma’s resistance to treatment. When it comes to the immune system’s role in this cancer’s proliferation, patients may hear researchers discuss its “low mutation burden.” What this means is that the cancer cells don’t look that different from the body’s non-cancerous cells on a genetic level. In other words, the number of gene mutations in a mesothelioma tumor are so few that the tumor looks like a normal cell to the immune system, which is in part how it evades it.
Based on scientific studies, the tumor mutation burden generally predicts the effectiveness of the immune checkpoint inhibitor therapy used for other cancers. The more mutations there are on the tumor that differentiate it from normal tissue, the easier it is for the primed immune system to see it and attack it, and the easier it is to target the tumor with therapies.
The flipside of this, of course, is that with mesothelioma that’s not the case, which begs the question: why do some mesothelioma patients respond to immunotherapy, while others don’t? What is so different about the ones who respond?
Tumor junction burden and antigen presentation as predictors of survival in mesothelioma
Researchers looked at 68 patients who had been treated with nivolumab and ipilimumab and nivolumab alone. Of these patients, 44 had sufficient DNA and RNA content derived from biopsy to be part of this analysis. What they concluded is that patients with a high tumor junction burden and antigen presentation survived longer than those without suggesting that it may be possible to use this information to select which patients might benefit from immunotherapy.
As mesothelioma treatment continues to head in the direction of targeted therapies, the expectation is that molecular and genetic knowledge acquired over the last decade will be incorporated into new generation treatment paradigms so doctors and patients can make fully informed decisions about treatment based on each individual patient’s circumstances.
A new worldwide clinical trial for mesothelioma is now open for enrollment
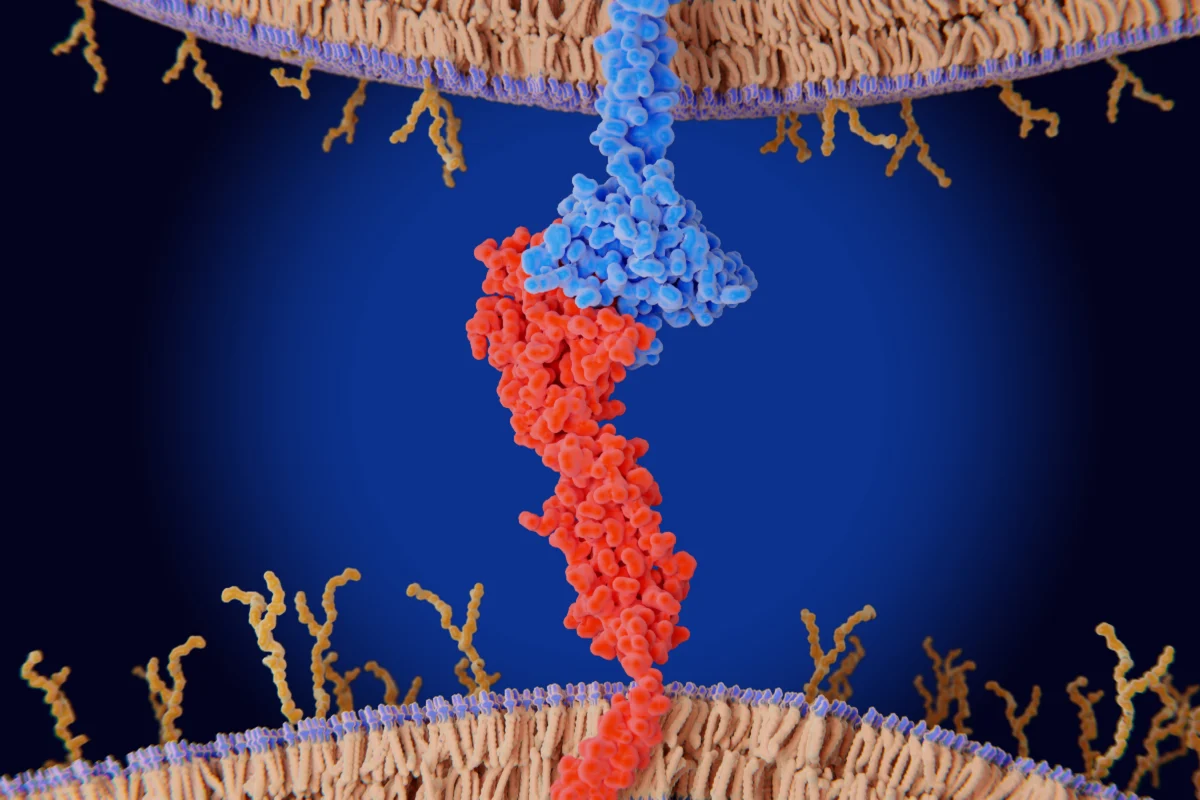
The “handshake” between the tumor and T cell prevents a T cell immune attack against mesothelioma. Disrupting the “handshake” holds the key to an immune response against this cancer. This Phase 3 immunotherapy clinical trial for mesothelioma tests a drug made to do exactly that and is now available to patients in the United States and across the world.
A new phase 3 clinical trial testing the efficacy of dual checkpoint inhibitor immunotherapy in combination with chemotherapy is now available to patients in the United States as well as around the world. The official name for the study is MEDI5752 in Combination With Carboplatin Plus Pemetrexed in Unresectable Pleural Mesothelioma and the shortened name is eVOLVE-Meso.
This AstraZeneca study tests a single immunotherapy agent called volrustomig in combination with standard chemotherapy against either standard of care chemotherapy alone or immunotherapy alone. The study builds on the recent FDA-approval of immunotherapy for mesothelioma which saw two agents, nivolumab (Opdivo) and ipilimumab (Yervoy), activate the immune system against cancer cells by binding to two receptors located on the T cell: the PD-1 and the CTLA-4. Single agent volrustomig targets the same two proteins, but the study also adds standard chemotherapy to its protocol.
How to inquire about enrollment?
The clinical trial is widely available at centers across the United States. A patient should contact their treating physician to discuss enrollment. Locations where the Evolve-Meso clinical trial is available are listed here: https://clinicaltrials.gov/study/NCT06097728#contacts-and-locations.
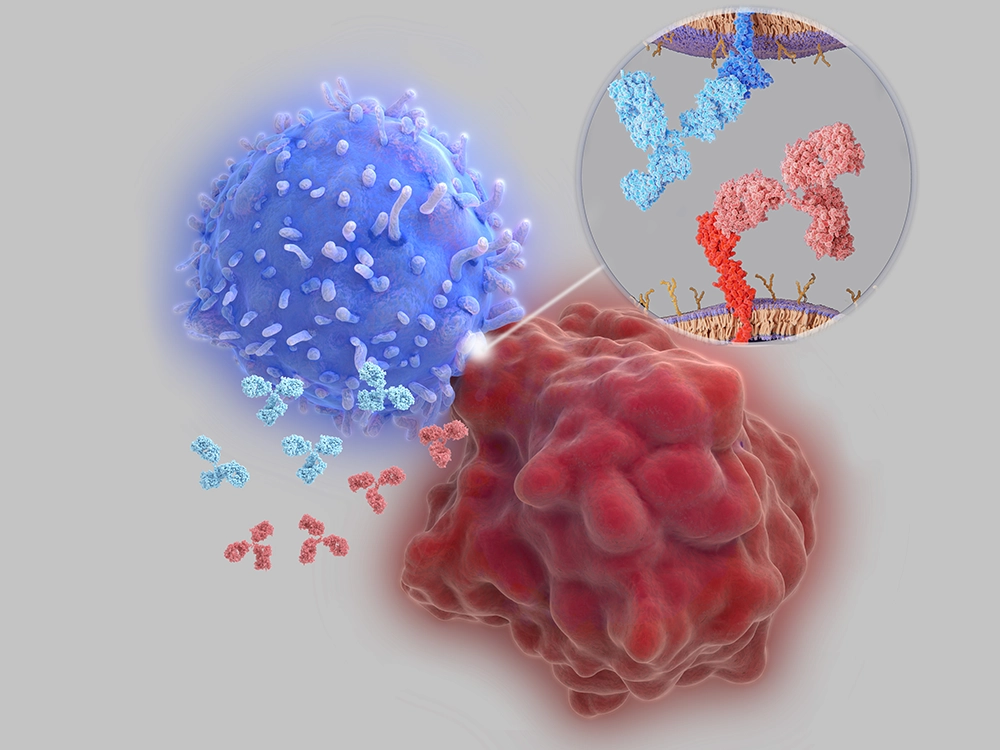
How does immunotherapy work to kill mesothelioma cells?
To understand how immunotherapy treatment works, we must first understand why the immune system tends to stay inactive against mesothelioma cells. Both the T cell and other cells, including tumors, express proteins. When certain proteins on the T cell bind to their counterparts on a healthy cell, this communicates to the T cell to not attack the healthy cell. This is an important preservation mechanism that prevents autoimmune reactions. So when the tumor’s proteins bind to the ones on the T cell, they tell the immune system not to attack which allows the cancer to proliferate. Immunotherapy medications act as a decoy binding protein that binds to either the T cell or the tumor cell, disrupting their ability to bind with one another.
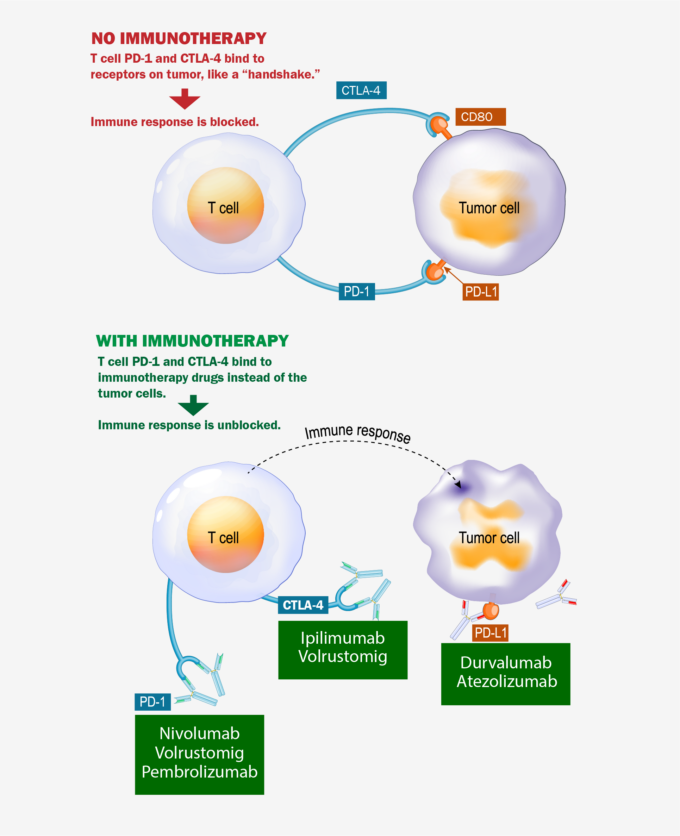
In the top part of this image, the T cell and the tumor cell connect causing no immune response against the tumor. In the bottom part of the image, the immunotherapy drugs connect to the expressed proteins on either the T cell or tumor thus inhibiting the connection between the two which in turn creates an immune reaction against the tumor. This is the basis of checkpoint inhibitor immunotherapy.
Immunotherapy + Chemotherapy: what is the rationale?
A common and valid question about combining chemotherapy with immunotherapy is: are we just throwing the kitchen sink at mesothelioma to see what sticks?
The answer is no.
There are, in fact, scientific reasons that would suggest that combining these two methods would lead to better results than administering them one at a time. Reason number one can be found in the answer to the question “why does the immune system not recognize mesothelioma as a foreign entity worth attacking from the beginning?” The answer is that mesothelioma cells’ receptors mimic those on the surface of healthy cells and they use the brakes built into the immune system to their advantage. But when chemotherapy is used to kill the cancer, the by-product of those dead cancer cells is seen as a foreign body by the immune system. So, adding chemotherapy to an immunotherapy regimen is one way to maximize the anti-tumor activity of both agents.
Timeline of FDA-approvals for mesothelioma
2004: Chemotherapy (Alimta/cisplatin)
2022: Immunotherapy (nivolumab / ipilimumab)
2024: Immunotherapy + chemotherapy for advanced mesothelioma (pembrolizumab also known by the brand name Keytruda, which is an anti-PD-1 agent, plus standard chemotherapy)
What is the difference between volrustomig and other immunotherapy agents used against mesothelioma
The volrustomig study is different from the 2024 immunotherapy (Keytruda) plus chemotherapy combination approval because volrustomig singularly binds to both the PD-1 and CTLA-4 receptors. Immunotherapy drugs targeting only the PD-1 or PDL1 receptors have shown to not be as effective as those also targeting the CTLA-4 receptor.
These two proteins, also known as checkpoint inhibitors, are located on the T cell. There, they play a crucial role in signaling to the immune system whether to attack the cancer cells or not. Without immunotherapy treatment, the tumor receptors (PD-L1 and CD80) bind to the reciprocal T cell receptors, signaling to the immune system not to attack the tumor. With immunotherapy that binds to them instead, the “handshake” between the tumor and the T cell is disrupted letting the immune system to attack the tumor.
Why should a patient consider participation in this study?
Mesothelioma patients have limited options for treatment available to them while the cancer is aggressive and moves fast. This study is an opportunity to try the combination of chemotherapy plus immunotherapy to potentially reap the most benefits.
What are the risks?
As with any study and/or treatment, one risk is that the treatment won’t work. With mesothelioma, this is a significant risk because the disease is quick and aggressive. However, over time, survival for mesothelioma patients has increased at least in part due to advancements in treatment options, and this study is one such option. Being a Phase 3 clinical trial, the drugs it uses have already been extensively studied for safety, but it is important to note that undergoing any type of immunotherapy can cause unintended immune reactions some of which can be life threatening. Speaking with the treating physician about potential risks and benefits is an important part of enrolling into a clinical trial.
What other treatments are in the works for mesothelioma?
Two other significant studies have been released in the last two years, both holding promise with regards to further treatment approvals. Both studies showed an improvement in survival in the most aggressive type of mesothelioma called the sarcomatoid subtype.
One of these studies combined Alimta/cisplatin (chemotherapy) with atezolizumab (immunotherapy) and also with bevacizumab (a VEGF inhibitor agent that limits vascular development leading to the tumor).
The other study, called ATOMIC, was successful in improving survival in the sarcomatoid and biphasic mesothelioma subtypes (most aggressive) by depriving the cancer cells of arginine, which is generally widely present in the most aggressive mesotheliomas.
Free Mesothelioma Patient & Treatment Guide
We’d like to offer you our in-depth guide, “A Patient’s Guide to Mesothelioma,” absolutely free of charge.
It contains a wealth of information and resources to help you better understand the condition, choose (and afford) appropriate treatment, and exercise your legal right to compensation.
Download Now